Background
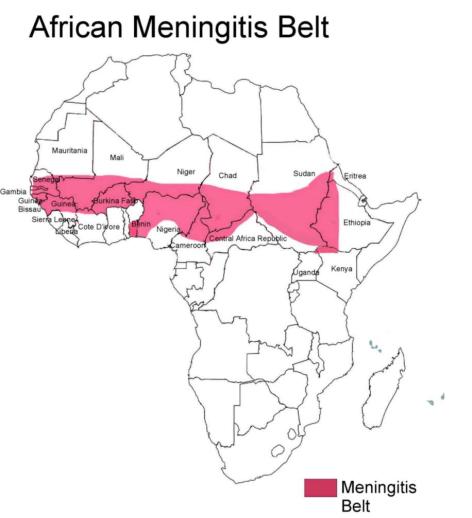
Ethiopia is one of the countries lying in the “African Meningitis Belt”. Meningcoccal meningitis in both endemic and epidemic forms, has been affecting Ethiopia for many years. Meningitis was first recorded in Ethiopia in 1902. Outbreaks were reported in 1935, in the 1940s, 1950s, 1964, 1977, 1981and 1989.
The 1981 and 1989 outbreaks were the most significant epidemics ever reported and documented, with the largest number of recorded cases and deaths. Nearly 50,000 cases and 990 deaths were reported during the 1981 epidemic and 45,806 cases and 1686 deaths in 1989. The overall attack rate in 1989 was 133/10,000 population and the case-fatality rate was 3.7%. About 70% of cases were between the ages of 5-44 years and affected more males. Unlike previous epidemics, the one in 1989 for the first time included areas outside of the traditional meningitis belt areas affecting regions as far south as Wollega in Oromiya Region.
Since the major outbreak in 1989, the disease did not reach an epidemic threshold for six years. At this time, there was a local outbreak of meningococcal meningitis in Konso wereda in the Southern Nation’s Nationality and People’s Region (SNNPR) on February 4, 1996 involving 771 cases and 11 deaths.
In 1997, three isolated outbreaks occurred again in SNNPR with a total of 319 cases and eight deaths between January and March. In 1999, an outbreak of meningitis occurred in Amhara and Tigray regions involving 268 cases and nine deaths between February and March.
In general, although sporadic cases of meningococcal meningitis occur every year, large epidemics in Ethiopia could be expected every 8-12 years. Since the last large epidemic occurred in 1989, the next cycle would have been expected between 1997 and 2001. It is also repeatedly shown that meningitis occurs during the dry season between late January and May. The most important Sero- Group in Ethiopia is Type “A” followed by type “C”.
Epidemic meningococcal disease in the meningitis belt countries occurs in cycles of 10 to 15 years. The last two epidemics in Ethiopia occurred eight years apart and were preceded within two to three years by epidemics in Sudan. The last major epidemic in Sudan occurred in 1999.
Current Situation
The current meningitis outbreak started in October 2000 in Quarit wereda in west Gojam zone in Amhara region and spread to districts adjacent to Quarit wereda and other districts in Amhara region. The outbreak further spread to SNNPR in the south, Gambella region in the west, Tigray in the north, Diredawa and Somali Region in the east.
The number of regions affected has increased from one in October to 10 in March with a total of 33 Zones and 93 weredas affected by end March.
The number of cases increased from 17 in October to 46 in November, 110 in December 590 in January 1,102 in February and 1,656 based on reports up until 24 March. To date 3,521 cases and 195 deaths have been registered. The case fatality rate is reported to be 5.6%.
The organism isolated in all areas of the outbreak is Nesseria Meningitidis serotype A, which is a major cause of meningitis epidemics in Africa. The age group affected shows that more than 80% of the cases are below the age of 30 years in all areas affected and 67% are below 15 years.
The majority of cases, some 52%, are reported from Amhara region followed by SNNPR, which reported 22% of the cases.
A recent field visit was undertaken by the Ministry of Health (MOH) and WHO to the two most affected regions, Amhara and SNNPR. The field visit included an assessment of Regional Health Bureau Zonal Health Departments, wereda health offices and health facilities in their response to the epidemic. The field visit identified the following two critical areas that require additional support.
1. Vaccinations
Since an appeal was made by the MOH in February, there has been a good response from partners. However, the remaining shortfall is still large and an urgent response is needed to control the epidemic.
2. Funding
The regions, zones, and weredas do not have a budget line for epidemic control, which limits their field activities including mass vaccinations. Lack of per diem for health workers, who are supposed to carry out the mass vaccinations at regional, zonal and wereda level, is a big constraint to the control of the epidemic.
Measures Taken So Far
The Ministry of Health, together with their partners, has carried out a coordinated response to controlling the epidemic. Steps taken thus far are as follows:
Coordination
At the central level, the Ministry of Health has established a partnership with WHO, UNICEF, MSF (Holland, Belgium, France, Switzerland) and the International Federation of the Red Cross with the Ethiopian Red Cross in order to coordinate the response to the epidemic. At regional, zonal and wereda level, epidemic control committees were revitalized and are working with regional health authorities.
Surveillance
The MOH gave surveillance a high priority, as it is crucial for monitoring the epidemic and for planning a proper response. The Ministry conducted a meeting with regional health authorities in January to strengthen the surveillance at all levels. At present, daily reporting from regions to the central level is in place. Similarly, each zone is reporting daily to their respective regions along with weredas through telephone and radio communications. The timely reporting of cases, though improved, still needs strengthening.Case Management
Guidelines on case management for meningitis have been distributed to all regions. However, distribution to health facilities has been limited due to limited regional capacity. Drugs for case management (Oily Chloramhenicol) has been supplied by WHO, and MSF to the national authorities. Most regions are reporting a shortage of basic drugs and supplies in health facilities.
Vaccinations
Since the outbreak started, vaccination strategies have been higly selective in affected weredas using limited stocks from the MOH and partners. This immunization strategy was slected instead of mass vaccinations due to vaccine shortages.
In February a major outbreak was imminent, as the number of districts reporting cases in excess of the threshold had increased. This prompted the Government to appeal for assistance from their partners and the donor community. The appeal identified the need for 6.7 million doses of meningiococcal vaccine A and C. The current strategy for vaccination plans to cover 80% of the population aged 2-30 years in the affected districts.
Support Needed
As one can see from the graph, the number of cases, which were very few in October, grew to a very substantial number by end March 2001. Ten of the eleven regional states and administrations are also affected. Over 50% of the zones and 20% of the weredas are affected. The vaccinations given to date have covered about 30% of the target population leaving a gap of 70%. In some areas, dry weather still continues to threaten the situation and the current trend of meningitis affecting people outside of the traditional meningitis belt will increase the demand for vaccines. This will mean more people who do not have past exposures to the organism are more likely to be affected. To avert a possible major epidemic it will be necessary to vaccinate at least 80% of the target population whose age ranges from 2-30 years. This will increase the number of protected people and create favourable conditions for arresting the transmission of the organism in the community. The appeal prepared by the Government in consultation with their partners was submitted to donors in February 2001. The response from donors and partners thus far has been positive. The table below shows the response by donors and the unmet needs. |
Item |
Requested |
Response |
Still Required * |
|
6.7 Million doses |
1,000,000
IFRC
500,000 UNICEF 500,000 WHO 400,000 MSF/B 350,000 MSF/F
110,000 MSF/CH 70,000 MSF/H Total 2,926,000 |
3,774,000 doses (or 75,480 vials of 50 doses with
auto distractible 10 ml syringes and needles and safety box) |
|
|
Local
cost/ Logistics for mass vaccination |
100,000 USD |
None |
100,000 |
|
Coordination/
Social mobilization /case management |
100,000 USD |
None |
100,000 |
* Detailed proposals are being prepared by the MOH and will include additional requirements such as drugs, vaccine carriers, and cold boxes.
![]()